














 18 / 22
18 / 22

© 2016, BSM Consulting
16
Basics of Glaucoma
•
The laser does not burn a hole through the eye. Instead, the heat causes some areas of the
trabecular meshwork to shrink, theoretically stretching adjacent areas open and permitting
aqueous humor to drain more easily.
•
Although the long-lasting effects of the procedure are patient-dependent, this procedure is often
considered when patients are noncompliant with their eye drops or are on multiple topical
therapies with poorly controlled intraocular pressures, but is sometimes considered earlier in the
treatment for some individuals.
Selective Laser Trabeculoplasty (SLT): Open-Angle Glaucoma
•
SLT is a laser procedure in which the laser targets intracellular melanin (pigmented cells). A
Nd:YAG laser is used for the procedure.
•
Unlike the precise targeting required by the ALT, the SLT shoots a large spot into the angle.
•
Results suggest that the procedure is safe and effective, with IOP results similar to those
through ALT.
•
The entire procedure takes less than 10 minutes, is usually painless, and is performed on an
outpatient basis using a topical anesthetic. Dilation of the pupil is not necessary, but constriction
of the pupil with a miotic agent (pilocarpine) is common.
•
Some suggest that due to less potential destruction to the trabecular meshwork tissues, the SLT
procedure might have more potential for repeat treatment than the ALT.
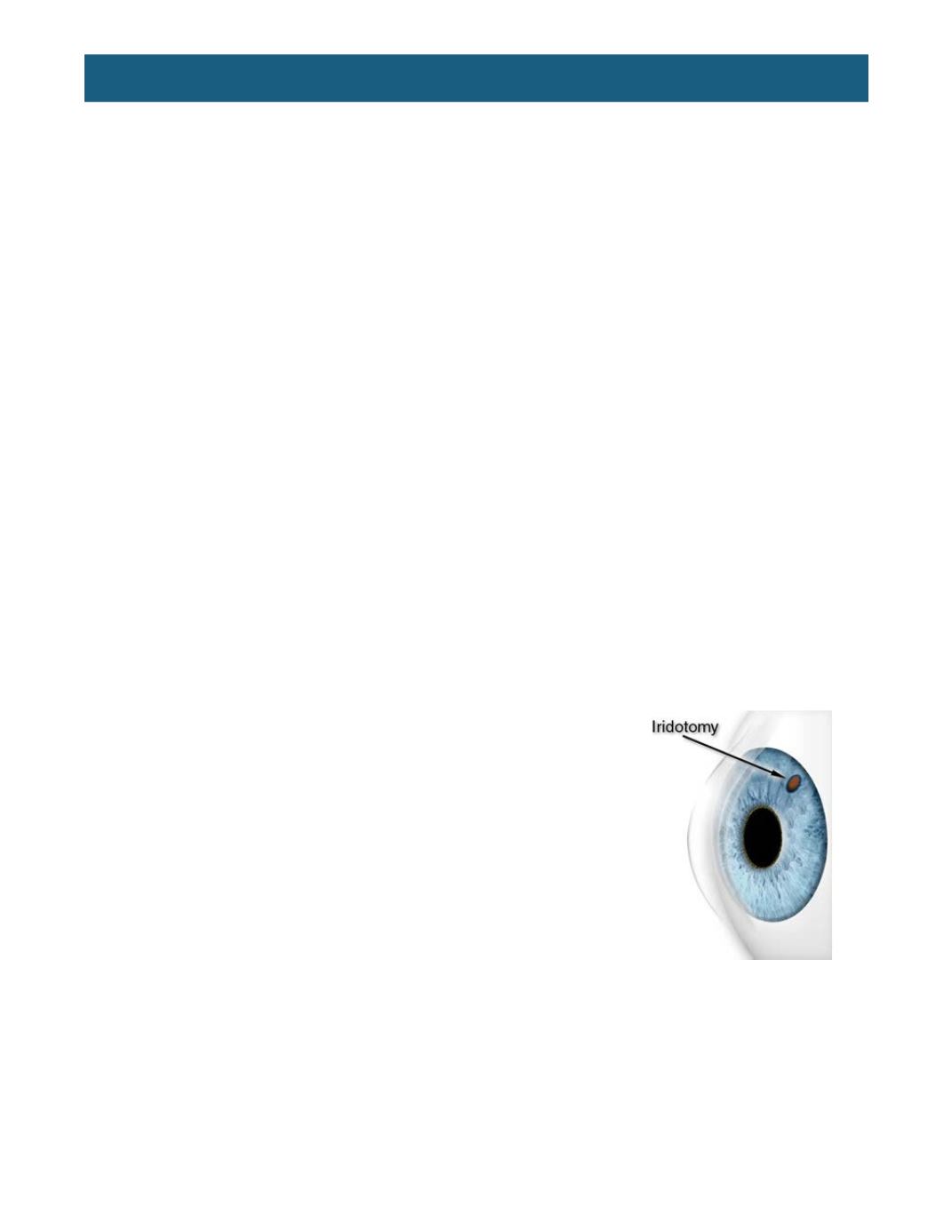
Laser Iridotomy: Narrow-Angle/Angle-Closure Glaucoma
•
Blockage of aqueous flow between the posterior and anterior chambers, or relative pupillary
block, the most common cause of angle-closure glaucoma. A procedure called laser iridotomy
can relieve this condition.
•
This surgery, which can be performed with the argon or Nd-YAG
lasers, creates a hole in the iris to allow free passage of aqueous.
The iridotomy is often located superiorly and is visible with the slit
lamp when the upper eyelid is lifted using a small beam of light from
the slit lamp through the pupil to retroilluminate through iridotomy.
Some prefer locating the iridotomy at 3 or 9 o’clock, and sometimes
the iridotomy is inferior if silicone oil is placed after a retinal
detachment.
•
Laser iridotomy can eliminate the chance of acute or chronic angle-
closure glaucoma in most eyes, and can eliminate chronic angle
closure in some.
•
Constriction of the pupil is often necessary prior to beginning the
procedure through the use of miotic drops or a hand-held light
source.
Argon Laser Peripheral Iridoplasty (ALPI): Angle-Closure Glaucoma
•
Under certain circumstances, laser iridotomy may fail to open a closed angle. If the angle is not
permanently closed with scar tissue, ALPI may help to open the angle.
•
This procedure is particularly useful in less common forms of angle-closure, such as plateau iris
syndrome or lens-related angle-closure.