












 6 / 22
6 / 22

© 2016, BSM Consulting
4
Modern Glaucoma Surgery
creating a hole from the anterior chamber into the space under the scleral flap. This is why the procedure
is called a trabeculectomy—because a small piece of the trabecular meshwork (trabecul-) is cut away (-
ectomy). Long before the trabeculectomy was developed, a full-thickness hole like this was allowed to
drain directly into the subconjunctival bleb. The problem with this older technique was that there was no
resistance to aqueous outflow, and the IOP tended to be too low to fully inflate the eyeball (called
hypotony). The trabeculectomy was designed to overcome this risk of low IOP by use of the partial-
thickness scleral flap. Returning to the trabeculectomy procedure, the scleral flap is now gently
repositioned in its scleral bed and loosely sutured back in place so the fluid exits the eye through the hole
in the trabecular meshwork but immediately encounters the underside of the scleral flap, which provides
just enough resistance to outflow to prevent hypotony. The fluid slowly oozes under the flap and emerges
into the subconjunctival space. The conjunctiva is resealed and a bleb should immediately form beneath it
(
Figure 1
).
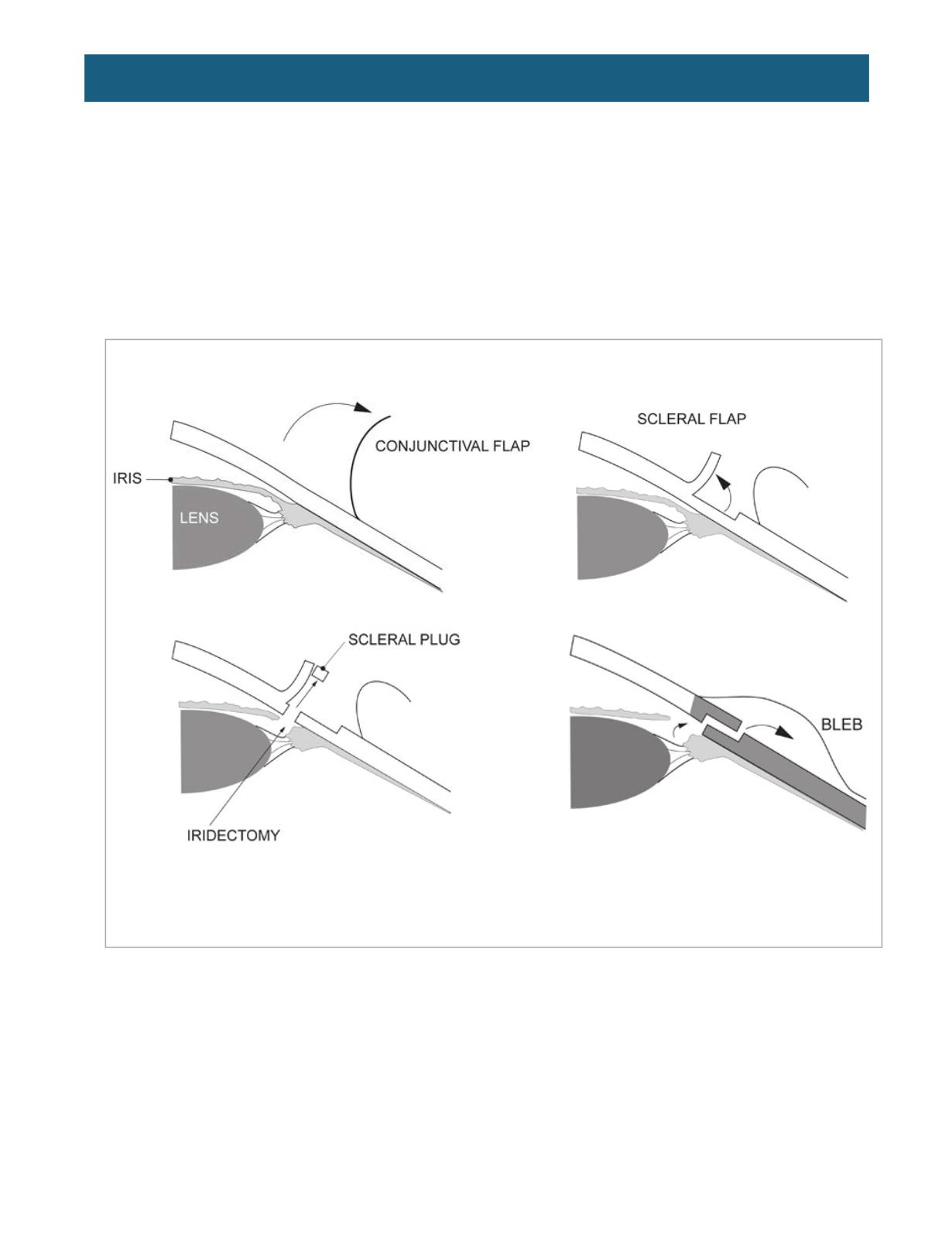
Figure 1.
Trabeculectomy technique.
Top left,
the conjunctival peritomy is created.
Top right,
the partial thickness scleral flap is created.
Bottom left,
the
hole in the trabecular meshwork and sclera is made.
Bottom right,
once the flap and conjunctiva are reapproximated,
aqueous flows through the hole, under the flap, and into the subconjunctival bleb.
(From
http://www.theglaucomaguide.com/book15trab.htm)
There are a few additional steps that are variably employed on a case-by-case basis. One is an
iridectomy. The hole in the trabecular meshwork made during trabeculectomy is positioned at the iris root.
The current of aqueous flowing through the hole can drag the peripheral iris into the new drainage hole,
plugging it and causing the procedure to fail. This occurs more commonly in phakic patients, and in
hyperopes who have smaller eyes. To prevent this complication, a small iridectomy can be performed
before sewing the scleral flap back into place; this removes the piece of iris that could otherwise plug the
new drainage hole.
Another optional step is the application of antimetabolites. When a hole is made in the eye, the body
naturally tries to heal itself and close the hole by forming a scar. There are several ways that healing
could cause the surgery to fail. The hole could heal shut, preventing aqueous from exiting the eye. The