












 15 / 22
15 / 22

© 2016, BSM Consulting
13
Modern Glaucoma Surgery
After the first visit, every surgeon has a different preferred schedule of follow-up visits, and the schedule
differs by procedure. For the minimally invasive trabecular bypass procedures often coupled with cataract
surgery, the standard cataract follow up of one day, one week, and one month may suffice. For the bleb-
based procedures, the follow-up schedule is often more intense. Some see the patient again the next
day, noting that endophthalmitis most commonly presents on the second day after surgery. Others will
see the patient back in five to seven days after the first visit. Thereafter, the follow-up schedule is dictated
by the clinical course, with patients typically seen once weekly for several weeks, then every other week
for several visits, and gradually extending the interval between visits until the typical three- to four-month
interval between regular glaucoma follow-up visits is re-established.
The ideal postoperative course for bleb-based procedures involves an intact bleb with no leaks, IOP
above the range of hypotony (generally >5 mmHg) and below the target IOP, with no evidence of
complications. This uncomplicated course is infrequently seen. More often, there are complications
related to the surgical procedure or the healing process that may or may not require intervention. The
technician should be looking for three things during postoperative workups: bleeding, infection, and
surgical failure evidenced by elevated IOP.
The most common postoperative complications and their management options are as follows:
•
Hyphema.
Blood in the anterior chamber is not uncommon following glaucoma surgery and
typically clears on its own. Large hyphemas may need to be surgically drained, but this is
uncommon.
•
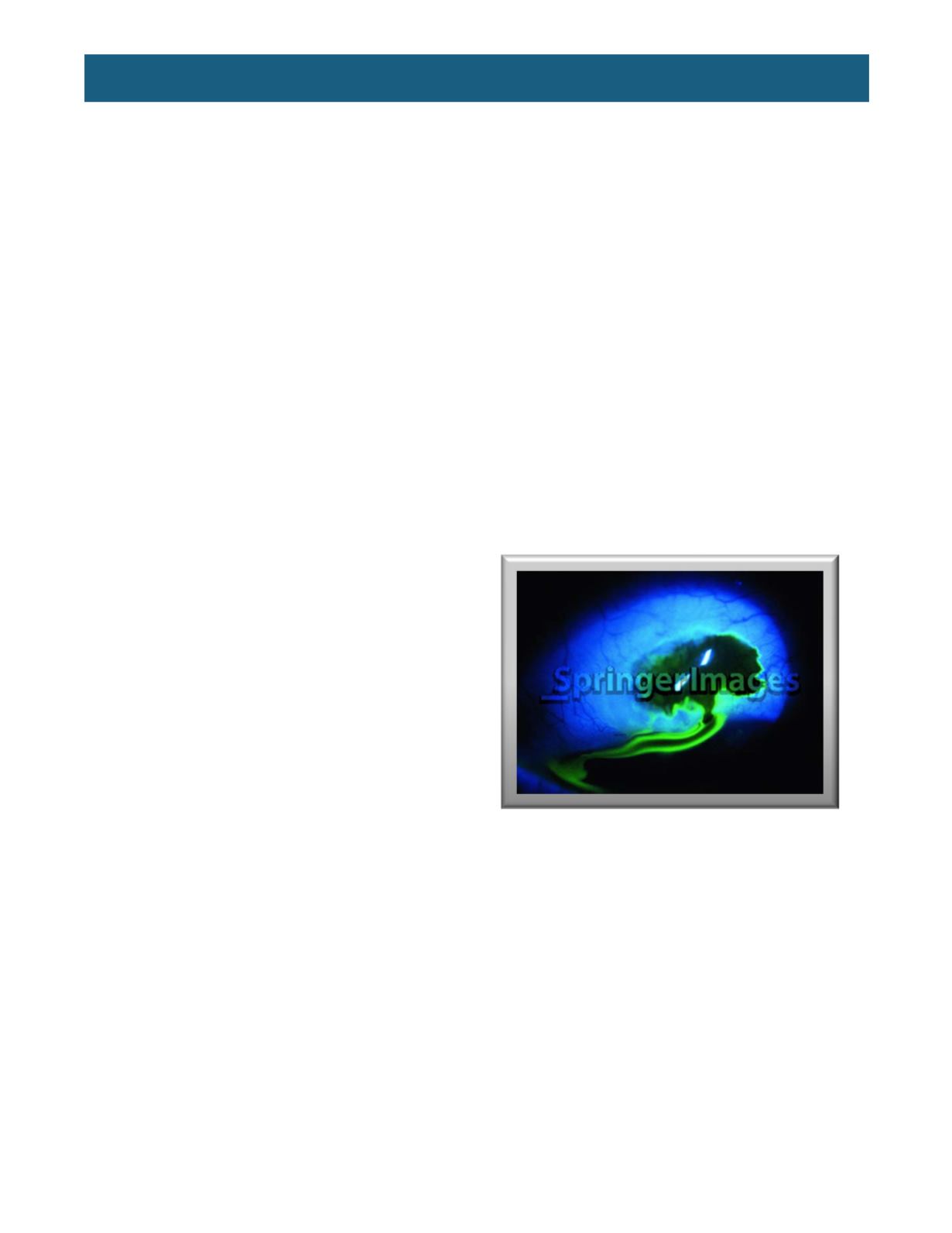
Wound leak.
A wound leak should be
suspected when the IOP is low, and the
bleb is also low. The appropriate test for a
wound leak is to paint the bleb with a
moistened fluorescein strip under blue light.
This is called a Seidel test, and when
positive, the strip will usually show a
pinpoint leak where the fluorescein is slowly
diluted by the escaping aqueous (
Figure 7
).
Wound leaks are common in the first
postoperative week and typically resolve
when the conjunctival incision heals closed.
If the leak is brisk and the anterior chamber
is shallow or flat, an oversized bandage
contact lens can be placed to put downward
pressure on the conjunctiva and scleral flap
to increase outflow resistance and to
blockade aqueous egress through the hole
in the conjunctiva. This is often coupled with
the addition of IOP-lowering medications that suppress aqueous production. This sounds
counterintuitive in an already low-IOP eye, but the goal is to reduce aqueous flow so that the hole
can heal, which it will not do if aqueous continues to flow through it. If this fails to resolve the bleb
leak, topical gentamicin is pro-inflammatory and a short course can accelerate healing/scarring to
close the hole, although at the risk of scarring the entire bleb. More invasive approaches can be
used if these more conservative measures fail. Blood can be drawn from a vein in the patient’s
arm and injected into the bleb. This will clot and temporarily stop the leak; blood also contains
molecules that promote healing so the conjunctival defect may heal while the clot blocks flow.
The argon laser can also be used to treat the conjunctiva around the hole; this promotes
inflammation which may accelerate the healing process. If all else fails, a return to the operating
room to suture the hole closed may be necessary.
•
Shallow or flat anterior chamber.
This is not uncommon in the early postoperative course and
usually resolves without intervention fairly quickly. Identifying the cause is critical. If the IOP is
also low, suspect a bleb leak (see previous paragraph) or, if the Seidel test is negative,
overfiltration caused by not suturing the scleral flap down tightly enough to provide appropriate
Figure 7.
A positive Seidel test indicating a bleb leak.
(From
http://www.springerimages.com/Images/RSS/1-10.1007_978-0-387-76700-0_70-13)